May 1996
| American Renaissance magazine | |
|---|---|
| Vol 7, No. 5 | May 1996 |
| CONTENTS |
|---|
Race and Health
Race, Slavery, and Blood Pressure
Race and Cancer
What Causes Infant Mortality?
Harlem v. Bangladesh
Book Review: The Color of Slavery
Book Review: One Black Master
O Tempora, O Mores!
Letters from Readers
| COVER STORY |
|---|
Race and Health
Racism is usually blamed for bad health among non-whites. The real causes are likely to be genetic.
by Arthur Holloway
On average, blacks are less healthy than whites and die sooner. They are more likely to die in infancy, get serious diseases, or die from accidents and murder. All of this is usually attributed to “racism” — either to direct harm caused by a prejudiced medical establishment or to the effects of the poverty and ignorance that are said to flow from racism.
In the medical literature, the higher rate of death for blacks — from virtually all causes — is called “excess deaths.” Every year, there are approximately 80,000 such “excess deaths,” or deaths that would not have occurred if blacks were as healthy and lived as long as whites. Calculations of this kind are often presented as measures of how racist American society is and how much blacks suffer on account of living in it.
Implicit in this measure, however, are three assumptions. One is that whites are the healthiest, most long-lived group, and are therefore the standard by which all others should be judged. Another is that all races have the same genetic potential for good health and long life. The third is that all races take equally good care of their health.
All three assumptions are false. To begin with, whites are by no means the healthiest Americans. Asians and Pacific Islanders (of which only five percent are Pacific Islanders) outlive whites by an average of seven years — exactly as long as whites outlive blacks. There are therefore 480,000 “excess deaths” among whites as compared to Asians, though no one seems to notice or care.
Secondly, science is steadily demolishing the view that races are genetically equivalent. For example, it is now well established that endemic malaria in West Africa resulted in genetic selection for blood abnormalities (technically known as hemoglobinopathies) that protect against malaria but can have dangerous side effects. Only blacks, therefore, get sickle cell disease and certain forms of thalassemia, which have indisputably genetic origins. It likewise appears that cancers behave differently, and more dangerously, in blacks than in whites for reasons that also appear to be genetic.
Finally, people of different races have different habits that affect their health. The U.S. Center for Disease Control reports that 38 percent of black women, 22 percent of white women, but only 10 percent of Asian and Pacific Islander women are overweight. The figures for men are blacks, 28 percent; whites, 25 percent; and Asians, 10 percent. The CDC also reports that American Indians and Alaska natives are heavy smokers. Forty-two to 70 percent of Northern Plains Indians and 56 percent of Alaska natives smoke as opposed to a rate of 29 percent for whites.
Nevertheless, in seeking the causes of racial differences in health and longevity, it is very difficult to untangle behavior, genetics, and environment. Some groups, for example, may be genetically predisposed to obesity or may become more easily addicted to nicotine. Smoking and obesity may be “environmental” factors that are mediated by genes.
Also complicating any analysis of causes is the fact that in all racial groups, the rich are healthier and live longer than the poor. Income therefore accounts for part of the health gap between whites and blacks and, because Asians have particularly high incomes, for part of the gap between Asians and whites. However, racial differences persist even when income is held constant; rich blacks die younger than rich whites, who die younger than rich Asians. Nor is income itself independent of genetics. Although wealth certainly buys good medical care, it also reflects traits that are associated with good health and long life: intelligence, discipline, and foresight.
Finally, medical and public health advances affect people of all races. During this century, life expectancy of both blacks and whites has increased by more than 30 years. Since 1915, white infant mortality has dropped from one in ten live births to fewer than one in a hundred. The black rate has dropped from one in six or seven to one in sixty. A black child born today has the life expectancy of a white child born in 1950.
Despite these complexities, there are racial differences in disease patterns that point strongly to biological rather social causes.
Infant Mortality
Much is made of the fact that the black infant mortality rate is more than twice the white rate. This is repeatedly cited as proof of “institutional racism,” and the poor medical care granted to blacks. However, there are plenty of racial groups in this country that have lower infant mortality rates than whites (below). The lowest are the Chinese and Japanese, who have higher incomes than whites, but Central Americans and even Mexicans — who have incomes almost as low as blacks — do as well or better than whites.
The graph below shows the percentage of mothers of each group who see a doctor during the first three months of pregnancy — the most common indicator of adequate pre-natal care — and the graph after that shows the percentage of different groups that do not have medical insurance. The second and third together show that prenatal care can be as much a matter of initiative as of formal medical coverage. Cubans, for example, are slightly more likely than blacks not to have medical insurance of any kind, but 80 percent of Cuban mothers (20 percent more than black mothers and slightly more than white mothers) manage to get first trimester treatment. In the United States there is medical care for any pregnant woman who wants it.
Mexican-Americans should have just about the highest infant mortality rates in America. They are almost as poor as blacks, less likely to finish high school, less likely to have insurance, and less likely to see a doctor during the first three months of pregnancy. They are also more than twice as likely as the rest of the population to give birth outside a hospital (2.5 percent of the time v. less than one percent). Yet, the Mexican-American infant mortality rate is slightly lower than the white rate (8.8 per 1000 births v. 9.0 per 1000 births) and well below the black rate of 18.7.
In terms of income and education, Puerto Ricans are comparable to Mexicans, with the difference that they are more likely to have medical coverage and to see a doctor during the first trimester. Yet their infant mortality rate is one of the worst in the country. Differences as consistent and dramatic as these suggest that races simply differ in their ability to survive the first year of childhood. All races respond to improvements in medicine and public health but inherent traits remain unchanged.
Another interesting indicator of health differentials is the rate at which people die from accidents. Although data for specific causes are available only for blacks and whites, the differences are significant. As a group, blacks are more likely to drown than whites. However, between the ages of one and four the likelihood is reversed because white children are more likely to be near residential swimming pools.
The usual explanation for the high rates at which blacks die in residential fires is that they live in decrepit houses without smoke alarms or fire escapes. However, it is significant that women of both races — who presumably live in the same houses as men — are considerable less likely than men to die in fires. This suggests a difference in temperament which may well exist between the races as well.
High rates among blacks of pedestrian death in auto accidents are not easy to explain in terms of poverty. Finally, it is hard to think of any explanation but greater recklessness for the fact that black men who own guns are five times more likely than white men who own guns to be involved in fatal firearms accidents (not shown on the chart).
Other data are available on accidental deaths from all causes for people of different races in the most accident-prone years: ages 15 to 24. American Indians die from accidents at a rate of about 90 per 100,000 or nearly twice the white rate of 55 per 100,000. Hispanics have a rate almost identical to whites, at 50 per 100,000, while Asians and Pacific Islanders have the lowest rate at about 32 per 100,000.
Hardy Asians
The two below tables show annual death rates per 100,000 population for the diseases from which people most frequently die. Men and women die from many of the same diseases but at different rates, so there is a table for each sex. The figures are adjusted by age, so that comparisons are between equivalent populations. Blacks, Hispanics, and Asians are all relatively young populations. Since mortal diseases usually strike old people, death rates must be adjusted by age so that non-white death rates do not seem artificially low.
Among men, blacks have the highest death rates for five of the eight diseases. Whites have the highest rate for two of the remaining diseases (both are heart diseases) and have the second highest rates, after blacks, for five diseases. Hispanics have the highest rate of cirrhosis. Asians and Pacific Islanders have the lowest death rates in all but one category — stroke — in which only American Indians have a better record.
For women, the situation is similar. Blacks lead in six out of nine diseases, and whites lead in two of the remaining three. Whites are second only to blacks in five out of nine diseases. Asians have the lowest rates in seven out of nine diseases and, again, are bettered only by American Indians, who have lower rates of stroke and colorectal cancer. For both sexes, adding up all the causes of death shows that there are far more “excess deaths” of whites by Asian or even American Indian standards then there are “excess deaths” of blacks by white standards. Presumably, this is of no importance.
The figures for Asians mask substantial differences between nationalities. Although Chinese, Japanese, Filipinos, Koreans and subcontinental Indians account for 80 percent of Asian-Americans and generally fit the health and economic patterns for this group, some Asian peoples do not. Poverty rates for Hmong (63 percent), Cambodians (43 percent), and Laotians (35 percent) are much higher than for Chinese, Japanese and Filipinos (6-8 percent), though the first three groups make up only 5.6 percent of the U.S. Asian population.
Southeast Asian men also smoke more than anyone else in America: Vietnamese (60 percent), Cambodians (71 percent), and Laotians (92 percent). Very little is known about disease rates for these subgroups, but they are likely to be much higher than for Asians as a whole. Pacific Islanders, who are “Asians” for statistical purposes, also bring down the average. Hawaiians, who account for 60 percent of the group, have a life expectancy lower than whites, as do Samoans, Guamanians, Tongans, and other islanders.
It makes no medical sense to treat Laotians and Samoans the same as Chinese or Japanese, but that is how the data are gathered. Including islanders and Southeast Asians increases death rates and infant mortality rates for “Asians and Pacific Islanders,” and means that the North Asian health record is even more impressive than this data suggest.
In general, American Indians come closest to Asians in their likelihood of dying from different diseases. This is not surprising, since they are thought to have crossed the land bridge from Asia only 35,000 to 40,000 years ago, and are closely related to North Asians. Probably the most important difference between the two populations is average IQ, which undoubtedly accounts for most of the differences both in income and rates of accidental death. That the two populations should have such different incomes, yet have similar disease rates is yet more evidence that racial biology plays a crucial role in health.
Figures for individual diseases also tell an interesting story. Cirrhosis is a degenerative disease of the liver that is usually caused by drinking, and high rates are normally a sign of wide-spread alcoholism. It is not surprising that American Indians have the highest rate of cirrhosis among women and the second highest rate among men. When mothers drink heavily during pregnancy, they can give their children a form of retardation known as fetal alcohol syndrome. The number of children born with this condition for every 10,000 births is much higher in Indians than in any other group: 30. The figures for others races are blacks — 6, whites — 0.9, Hispanics — 0.8, and Asians — 0.3.
Indians also smoke more than everyone but Southeast Asians, but have the second-lowest lung cancer rates. They die from smoking-related cancers (lung, esophagus, larynx) at about half the white rate. Indians may well have a genetic resistance to lung cancer just as they have a predisposition to alcoholism.
Hispanics, many of whom are genetically related to American Indians, also seem to resist lung cancer. Although about 40 percent of Mexican-American men smoke, compared to 30 percent of white men, Mexican-Americans have about half the rate of lung cancer.
Blacks do not seem to enjoy any particular immunity. Thirty-four percent of adult blacks (as opposed to 29 percent of adult whites) smoke, and 78 percent of black smokers (as opposed to 56 percent of whites) smoke high-tar cigarettes. Blacks are also three times more likely than whites to smoke menthol cigarettes (76 percent v. 23 percent). Blacks have the highest smoking-related cancer rates of all Americans (27 percent higher than whites), and smoking is thought to account for 20 to 30 percent of all low birth weight babies in America and 10 percent of all infant deaths.
Diabetes appears to be strongly influenced by genes. The Pima tribe of American Indians has the highest rate — 50 percent — of any population in the world, and Indians in general have high rates. Blacks have even higher rates, which may be aggravated by eating habits. Every year, the average black household spends 54 percent more than the average white household on sugar. Likewise, blacks are the greatest consumers of premixed cocktails, wine coolers and other sweet drinks. Although the sugar-sweetened version of Kool-Aid claims to have 25 percent less sugar than Coca-Cola or Pepsi-Cola, blacks prefer to buy the unsweetened version and add lots of sugar.
Asians are less likely than whites to suffer from serious diseases, but there are a few exceptions. One is diabetes. Asians are more likely than whites to have the disease but less likely to die from it. Asians seem to get a less deadly or slower-acting form. Also, curiously, Asians are twice as likely as other groups to suffer from motion sickness.
Tuberculosis, though rarely fatal, is another disease from which Asians suffer at greater rates than any other group (though it would be interesting to know how much the group average is driven up by Laotians and Vietnamese). Asians are ten times more likely than whites to get tuberculosis and the figures for other groups are blacks — eight times more likely, Hispanics — five times, American Indians — 4.5 times. More than two thirds of all cases occur in the 25 percent of the population that is non-white, and nearly one third of the non-whites who get tuberculosis were born outside the United States.
There appear to be distinctly different racial susceptibilities to tuberculosis. A study of 165 racially integrated nursing homes in Arkansas found that although all patients were free of the disease when they were admitted, blacks were twice as likely as whites to become infected.
Another condition that varies by race for what are probably genetic reasons is osteoporosis. Older women who do not get enough calcium are especially prone to it, but whites suffer more than anyone else. Hip and other fractures are most common in northern European women, despite the fact that they consume more calcium than all other groups. The most likely explanations are genetically determined differences in bone accretion and bone characteristics, as well as differences in vitamin D metabolism.
Glaucoma affects blacks at five times the white rate and strikes blacks earlier. This difference is independent of socioeconomic status or access to medicine and is likely to have a genetic cause. Glaucoma is the leading cause of blindness among blacks.
Venereal diseases show starkly divergent incidence rates. Among blacks, syphilis rates per 100,000 population have soared since the introduction of crack cocaine in 1985, climbing from 50 to 140 in the five years to 1990. During the same period, the white rate declined from three to two per 100,000, which means blacks are 70 times more likely to have syphilis than whites. The 1990 figure for Hispanics is 20 per 100,000, or ten times the white rate.
Curiously, gonorrhea appears to have been unaffected by crack cocaine; from 1985 to 1990, the black rate hovered around 2,000 per 100,000 population. In 1990, that was approximately 100 times the white rate and the Hispanic rate was approximately four times the white rate. Blacks are more promiscuous than whites and less likely to take precautions against venereal disease. There appears to be no research on whether genetic reasons also account for such enormous racial differences in infection rates.
Blacks and Hispanics have higher rates of AIDS than whites, who have higher rates than Asians. Three percent of black men between the ages of 27 and 39 have the HIV virus. The figure for Hispanics is 1.7 percent and for whites it is 0.7 percent. Blacks and Hispanics — especially women — continue to contract AIDS at ever-increasing rates. Three quarters of the American women who have AIDS are non-white, as are fully 84 percent of the children who contracted it from infected parents.
r-K Theory?
With only a few exceptions, disease and death rates support the life-history theory of racial differences proposed by Prof. J. Philippe Rushton of the University of Western Ontario. To put it in far too small a nut shell, Prof. Rushton argues that of the major racial groups Asians live the longest, have the largest brains, are least preoccupied with sex, and devote the most energy to rearing small families rather than siring large ones. Whites are second to Asians, followed by blacks.
The rates at which members of different races contract and die of diseases is perfectly consistent with this pattern of what are known as r-K variables. Blacks have the highest disease and death rates, followed by whites, followed by Asians. Some races simply appear to be biologically designed to live longer than others.
Except in rare cases, it is difficult completely to isolate the biological causes of racial differences in disease rates, and some differences that seem to be biological may have unknown environmental causes. However, biological interpretations are greatly bolstered by the fact that they fit almost perfectly into the r-K pattern that Prof. Rushton has discovered. The human genome project will eventually supply the answers; in the meantime, it is a safe bet that race, not “racism,” explains most differences in disease and death rates.
| ARTICLE |
|---|
Race, Slavery, and Blood Pressure
It has been known since the 1930s that blacks are more likely to have higher blood pressure than whites. Hypertension, which clearly has a genetic component and runs in families, is associated with heart disease, stroke, hardening of the arteries, and hypertensive kidney failure. Blacks die from all of these diseases more frequently than whites. Since stress can increase blood pressure, this difference has frequently been blamed on racism.
In fact, blacks show physiological responses that contribute to high blood pressure. In one experiment, blacks and whites who were carefully matched for age, sex, diet, medical history, and fitness levels were given a mild but harmless stress test in which they had a hand packed in ice for 30 seconds. The normal reaction is for blood vessels to constrict; however, blacks’ vessels stayed constricted — thus elevating blood pressure — for ten times longer than those of whites.
A salty diet can increase blood pressure. Blacks and whites have essentially the same levels of salt intake, but blacks retain salt for a far longer period than whites before excreting it. Blood pressure in blacks also rises and falls much more rapidly in response to changes in salt consumption. Similarly, blacks with high blood pressure respond more readily than whites to diuretic drugs, which cause the kidneys to excrete salt. Whites respond more readily to so-called beta-blockers, which reduce heart rate and heart output.
It has recently been discovered that blacks have less flexible blood vessels than whites. Their arteries do not dilate as well as those of whites, and dilation helps blood circulate more rapidly when there is high demand for it. Blacks may compensate by increasing blood pressure.
Blacks are more likely than whites to suffer from a thickening of the heart muscle, which may increase the risk of heart disease. Blacks also tend to to behave in ways that increase blood pressure: They are more likely than whites to smoke, not get much exercise, not eat enough calcium, and get fat.
On the other hand, American blacks tend to have higher blood pressure than West Africans, which is more grounds for the racism theory. However, blacks in Jamaica, which is black-run and overwhelmingly black, also have black-American levels of blood pressure. The explanation may lie in the rigors blacks faced when they were captured and shipped to the New World as slaves.
Virtually all slaves were captured during tribal wars in the African interior. It is estimated that 25 percent did not survive the march to the coast. Another 12 percent are thought to have died in holding pens, or barracoons, waiting for white slave traders. The passage to the New World is thought to have killed another 10 to 15 percent.
The most common cause of death was probably diarrhea, in which the victim dies from a sudden, massive loss of salt and water. It may be that blacks who survived capture and the middle passage were selected for an unusually high ability to retain salt, which could explain why New World blacks have higher blood pressure than Africans.
| ARTICLE |
|---|
Race and Cancer
Blacks get most cancers more often than whites and are less likely to survive them. Five years after a cancer diagnosis, 50 percent of white men are dead; 65 percent of black men are dead. Women survive better than men. Five years after diagnosis, 40 percent of white women and 55 percent of black women are dead.
Survival rates are no doubt influenced by quality of medical treatment. However, studies of a number of cancers show that even under rigorously identical circumstances cancer seems to follow a more deadly course in blacks. For example, even when breast cancer is diagnosed at the same stage and treated the same way, blacks are more likely to die from it. Their cancers tend to grow more rapidly, to contain more malignant cells, and to be impervious to hormone treatments.
Blacks are likewise more likely to get prostate cancer. Like breast cancer, it attacks blacks more aggressively and at an earlier age than it does whites. A study of blacks and whites in the military, who were matched for health and medical profiles, found that identical screening methods picked up more cases in blacks, but that identical treatment worked better on whites. Scientists have now identified certain markers in the 5-alpha reductase gene that occur only in blacks. This gene is believed to regulate cell division in the prostate, and the markers are associated with the disease.
High rates of cancer among blacks are a cause of considerable national concern and have prompted a number of studies. In fact, as the graph near the top of the page shows, by the standards of most racial and ethnic groups, whites have disturbingly high rates of prostate cancer, as they do of many other diseases. So far, this seems to be of little interest to the research community.
| ARTICLE |
|---|
What Causes Infant Mortality?
During the 1950s, the United States ranked sixth in the world in infant mortality. During the next three decades, infant mortality declined but not as quickly as in some other countries. By the mid-1980s, the United States was ranked 22nd in the world. During the same period, the black American infant mortality rate declined more slowly than the white rate. In the 1950s, blacks were 60 percent more likely than whites to die in infancy, but 30 years later they were more than twice as likely to do so. This difference explains much of the United States’ decline in world rankings.
The single most important indicator that a new-born will not survive the first year is low birth weight (LBW), defined as anything less than 2,500 grams. In the 1960s many people thought poor nutrition was the main cause of LBW and of infant mortality. In 1972, Congress duly established the Special Supplemental Food Program for Women, Infants and Children (WIC), under which the government gives women who are pregnant or have small children 100 percent of their protein and 50 percent of their calorie requirements. Children up to age four get virtually all the food they need.
To be eligible, women and children must be at “nutritional risk” — a capriciously defined condition — and must have family incomes no more than slightly less than double the poverty level. Nearly one third of the four million babies born each year now eat WIC food at a cost of $2.5 billion a year in federal money plus distribution costs borne by the states.
WIC is an untouchable program; no one dares take the crust from the babe’s mouth. However, malnutrition has virtually nothing to do with low birth rate and infant mortality. Seventy percent of LBW babies are premature and other medical or accidental causes account for most of the rest.
The United States has higher rates of premature birth than virtually any other country, rich or poor. LBW is much more common in places like Bangladesh, Guatemala, or black Africa than in the United States, but in those countries it actually is caused by malnutrition. However, poor countries have lower rates of premature birth. Jamaica, whose population is almost all black and poor, has a substantially lower infant mortality rate than does Washington, DC.
In the United States, therefore, infant mortality is mainly caused by LBW due to early birth, not malnutrition or bad medical care. American mothers are adequately fed and American hospitals are better at salvaging underweight babies than any in the world. What causes premature birth?
It is disproportionately a black problem. The black LBW rate is more than twice the white rate and has risen steadily since 1979, while the white rate has dropped or stayed level. Behavior appears to account for some of it. Smoking, drug use, and previous abortions all contribute to premature birth. Twice as many blacks as whites (24 percent v. 12 percent) use alcohol, tobacco or drugs during pregnancy (as opposed to nine percent for Hispanics and seven percent for Asians). Venereal disease — also vastly higher in blacks than in whites (see main article) — infects the genital tract and the membranes that surround the baby.
Probably the worst culprit is crack cocaine, which is well known to cause early birth. Some pregnant crack addicts smoke more than ever in order to end the inconveniences of pregnancy more quickly. Black mothers are reportedly eight times more likely than whites to test positive for cocaine in their blood at the time they give birth.
On the other hand, low birth weight in blacks is probably not due entirely to behavior. The normal gestation period for blacks is slightly shorter than that for whites, just as the period for whites is slightly shorter than that for Chinese, Japanese, and Koreans. The normal black infant is therefore likely to be smaller than that of other races — risks inherent to lower birth weight are only exacerbated by parental behavior. After they are born, black infants actually do face a wholly unnecessary “nutritional” disadvantage: Of all racial groups they are the least likely to be breast-fed. This means not only that they are more likely not to get the best known food for new-borns; black mothers are also more likely than other mothers to misuse infant formula by thinning it with too much water, mixing it with oatmeal, or even diluting it with Coca-Cola.
Simply persuading black women to nurse their babies would probably do more good than billions of dollars in WIC food.
Arthur Holloway is the pen name of a self-employed academic living in the midwest.
| ARTICLE |
|---|
Harlem v. Bangladesh
It caused a considerable stir when the New England Journal of Medicine first reported in 1990 that men in Bangladesh have a better chance of living to age 65 than men in Harlem. As the accompanying graph shows, it is actually at age 45 that the percentage of men still surviving in Bangladesh begins to exceed the percentage in Harlem.
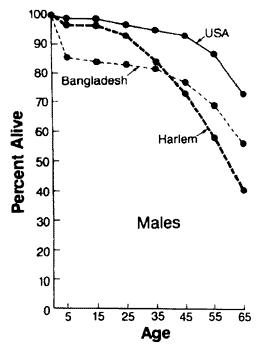
The different shapes of the curves for Bangladesh and Harlem say a great deal about the two locales. Infant mortality and childhood diseases are far greater scourges in Bangladesh. A child born in Harlem benefits from advanced medicine, and is therefore much less likely to die before age five than a Bangladeshi.
It is between ages 25 and 45 that survival rates plummet in Harlem. Homicide, accidental death, and drug overdoses start cutting men down at a greater rate than in virtually any other place on earth.
The irony is that the abbreviated life expectancy in Harlem was first publicized as yet more evidence of the heavy price blacks pay for living in America. In fact, the high survival rate in the early years is a huge advantage blacks gain from living among whites. Subsequent death rates are largely a result of black behavior and susceptibility to disease.
| BOOK REVIEW |
|---|
The Color of Slavery
Simon Legree dons a new face.
Black Slaveowners: Free Black Slave Masters in South Carolina, 1790-1860, Larry Koger, University of South Carolina Press, 1985, 286 pp., $14.95 (newly released in paperback)
reviewed by W. Scott Wilson
The myth persists that slavery consisted solely of cruel white masters and exploited blacks. This history of oppression is supposedly responsible for all the troubles blacks face today and, for some blacks, it even justifies reparations. Few people realize that black Americans owned slaves, too. In Black Slaveowners, Larry Koger has written a meticulously researched account of the black, slave-owning elite of South Carolina.
Mr. Koger’s purpose is not just to describe the black slaveowning class but to refute the majority academic view that blacks purchased other blacks — primarily their own relatives — in order to set them free. Mr. Koger believes that blacks generally bought, owned, and sold other blacks for economic reasons, just as whites did.
Before the War Between the States, black slaveowners could be found in every slave state and at nearly all educational and economic levels. Mr. Koger reports that, according to the 1830 census, black masters in just four states — Louisiana, Maryland, Virginia and South Carolina — owned more than 10,000 slaves. Even the enlightened state of New York was home to eight black slaveowners. In the South, many pro-slavery whites grew to accept these men and women as neighbors and as allies against abolition.
Mr. Koger reports that by 1840, South Carolina boasted 454 Negro masters with 2,357 slaves. Although only about one in five white households in the South owned slaves, approximately 75 percent of the free black heads of household in the state owned slaves. Many former slaves did not regard slavery as a malevolent institution but as an economic opportunity, and had no qualms about buying other blacks once they were able to.
Who were these black slaveowners? Eighty-three percent were mulattoes, even though they accounted for only 49 percent of all free blacks. Ninety percent of their slaves, by comparison, were of unmixed African descent. A few mixed-race masters inherited slaves from a white parent or grandparent, but most worked and saved on their own to acquire their property.
Mulattoes as a group eventually came to shun all dark-skinned blacks, slave and free, whom they viewed as beneath them. According to the 1860 census, nine out of ten mulattoes chose mixed-race spouses. Their dislike for darker blacks was so pronounced that if a free mulatto woman could not find a mixed-race free man to marry, she might marry a mulatto slave rather than a free black.
Mulattoes had advantages that were both social and biological. Between 1800 and 1840, the average earnings of the wealthiest free, dark-skinned blacks was only $1,805 while the mulatto elite’s average came to $4,642. To highlight the differences, mixed-race blacks of South Carolina formed the Brown Fellowship Society. Membership was limited to “free brown men” (mulattoes) and included a number of slaveowners.
Some free mulattoes kept their distance from blacks for fear of being mistaken for slaves. Others strongly identified with whites and wanted to preserve the right to own slaves. During the War Between the States many mulatto slaveowners wholly supported the Confederacy. One wrote to his white associates: “in our veins flows the blood of the white race, in some half, in others more than half . . . our attachments are with you, our hopes and safety and protection from you . . . our allegiance is due to South Carolina and in her defense we will offer up our lives, and all that is dear to us.”
After the war, when the fear of being mistaken for a slave had past, mulattoes continued to see themselves as above pure blacks. According to Mr. Koger, they refused to attend church with them and even tried to set up a caste system based on pre-war social strata.
It may be that relations between Charleston’s mulattoes and full-blooded blacks were permanently soured by events that took place between 1818 and 1822. With the help of 4,000 sympathetic slaves, a free black named Denmark Vesey plotted to lead the blacks of Charleston in a violent uprising. Vesey’s supporters had located stockpiles of weapons to seize. One slave vowed he had access to “a keg of Powder and five hundred (500) muskets.”
The plan was not just to fight for freedom but to kill every white in the city. For blacks who felt hesitant about butchering whites, Vesey invoked Old Testament parallels to God’s chosen people exterminating their enemies. A religious eclectic, he also entreated one co-conspirator, an Angolan mystic named Gullah Jack, to produce a magic potion to protect the rebels from harm. He further inspired his followers by recounting how the blacks of Santo Domingo rose up, massacring scores of white families in the name of freedom.
Vesey excluded free blacks from his plan. All of his closest accomplices were, unlike himself, slaves. Vesey, who was born and “nurtured in the bosom of Africa,” also kept mulattoes out of the plot because of their ties to whites and the slaveowning class.
The divisions among Charleston blacks were so complete that Vesey was able to keep his plans secret for four years. Ultimately, it was a mulatto slave who betrayed the insurrection just two weeks before it was to start. South Carolina’s Governor asked for federal troops to protect the city. Then Secretary of War, John C. Calhoun, dispatched them, and all the rebel leaders were arrested within two weeks.
The plot — and its betrayal — deepened divisions between blacks and browns. Both groups used the event to justify their suspicions of the other and it may have removed the doubts of some free mulattoes about owning human property.
The Woodson Thesis
Black slavemasters are an embarrassment to the orthodox, and have generally been justified by means of “the Woodson thesis.” In 1924, historian Carter G. Woodson hypothesized that blacks were “benevolent” owners who bought spouses and relatives for the purpose of freeing them. Mr. Koger’s analysis refutes this claim. He has discovered that 65 percent of purchases of slaves by blacks in the city of Charleston were clearly motivated by profit and only eight percent could be called “benevolent.” He could not determine the motive for the remaining 27 percent.
Several benevolent transactions are detailed in the text, including one 1817 purchase by a black man of his wife. Interestingly, for reasons Mr. Koger does not appear to know, the man kept his wife as a slave for two years before freeing her.
From 1820 until the war, the South Carolina legislature began limiting manumission to extraordinary circumstances, such as life-saving heroism. This made it even less likely that free blacks would buy slaves in order to free them, because it became next to impossible to do so. A few, though, did find ways around the new laws by deeding their slaves to friends or sympathizers with a written agreement that the slaves be allowed to live as if they were free. Some of these nominal slaves worked for wages and paid taxes. One, Hannah Gonzales, even bought and sold slaves herself.
“Benevolent” ownership was unusual because, as Mr. Koger often points out, black slaveowners felt little pity for slaves. Some historians have been misled by the large number of black slave holders who did purchase relatives. Many, though, bought additional slaves for strictly economic reasons. Mr. Koger surmises that for them, “slavery was an oppressive institution when it affected a beloved relative or a friend, but beyond that realm, slavery was viewed as a profit-making institution to be exploited.”
Black slaveowners took an entirely business-like attitude towards their property. They went to court to fight for their ownership interests, and appear to have been no more likely than whites to free slaves in their wills. Like whites, blacks used their slaves as collateral; one slaveowner in Charleston even mortgaged her two children, born as slaves, to secure a debt.
Like all careful students of slavery, Mr. Koger finds that it was not always the harsh existence modern portrayals suggest. Would Alex Haley’s fictional character, Kunta Kinte, have dared a dangerous escape to return to his master if he had been captured by the British during the Revolutionary War? Mr. Koger tells of one slave who did. He reports that, contrary to what is usually believed, many former slaves “harbored no ill feelings toward their former masters and showed no signs of deep hatred for the institution that enslaved them.”
Blacks, like whites, could nevertheless be cruel masters. It was not uncommon for black slaveowners to throw insubordinate servants in jail or the workhouse for up to thirty days, and flog them severely when they got out. If a recently purchased slave was unruly, the owner would often resell it, using the proceeds to buy more compliant property.
Blacks owned slaves until the fall of the Confederacy. Even in 1864, during the darkest days of the war, half of Charleston’s black slaveowners who had owned slaves in 1860 still owned them. In the early 1860s, some blacks felt optimistic enough to purchase slaves for the first time. In the final months of the war, many black slaveowners either tried to sell to whomever would buy or persisted in using their labor until the conquering Union armies forced them to stop. Very few willingly emancipated their property. As Mr. Koger writes, “the colored masters of Charleston perceived the invasion as apocalyptic destruction rather than salvation.” He estimates that emancipation cost Charleston’s black masters $216,000 in slave-property — a large loss for just one city.
Black Slaveowners is a fascinating look at a misunderstood era of American history, but Mr. Koger is sometimes a little too free with his personal opinions, especially about would-be mass-murderer, Denmark Vesey. We learn that Vesey had “a certain sparkle in [his] eyes” and was wealthy enough to own slaves had it not been for the “racial pride [that] ran through his veins.” After his conviction, he “fac[ed] the gallows with courage.” Mr. Koger sums up, with these words, the man who planned the murder of every white man, woman, and child in Charleston: “Denmark Vesey showed his followers in life how to be a proud black man, urging the slaves to be men and to take their freedom; he also showed them how to die with conviction.”
Nevertheless, Larry Koger’s study of black slaveowners and his refutation of the theory of “benevolent Negro slaveowners” is as welcome as it is well researched. His investigations may force scholars to revise their assumptions about the peculiar institution and its supporters.
W. Scott Wilson is Assistant Editor of American Renaissance.
| BOOK REVIEW |
|---|
One Black Master
Andrew Durnford: A Black Sugar Planter in the Antebellum South, by David O. Whitten, Transaction Publishers, 1995, 133 pp., $29.95.
reviewed by W. Scott Wilson
What was life like for a black slaveowner? In Andrew Durnford, David O. Whitten has drawn on the correspondence between a free, mulatto master and his lifelong white friend to give us a glimpse into a forgotten corner of the American past.
Andrew Durnford was said to be the child of a free black woman and her wealthy English lover, Thomas Durnford. Thomas gave his son an aristocratic education that included French, mathematics, and medicine. Although the most that illegitimate mulatto children could usually hope for was freedom upon the death of their fathers, Andrew inherited both Thomas Durnford’s name and a portion of his estate. He subscribed to periodicals in both French and English, and valued education enough to send his own son to Lafayette College in Pennsylvania.
John McDonogh had been a close friend and business partner of Durnford’s father, Thomas. When Thomas Durnford died, owing almost $10,000 to McDonogh, McDonogh was granted curatorship over the estate. His association with Durnford’s son was a crucial advantage to the young mulatto. In 1831, McDonogh set up Andrew Durnford as a planter, selling to him — on credit — 14 slaves and 672 acres of land along the Mississippi. McDonogh clearly had an abiding affection for Durnford and appears to have treated him as a social equal. He helped Durnford acquire yet more property, and by 1835, Durnford owned 77 slaves and more than 1600 acres of land.
Durnford was not a successful businessman. He was able to cover the costs of running his plantation for only two out of 26 years. He owned more slaves than he needed and, according to Mr. Whitten, “would have enjoyed greater financial returns had he put his capital out at interest and employed himself at salary.” He lived comfortably, but depended on the kindness of his creditor. When he died he still owed $13,000 to John McDonogh’s survivors.
Mr. Whitten writes that Durnford was a kindly master, but he appears to have had no illusions about his property. On one occasion he wrote of his “rascally Negroes,” saying “I have to threaten them severely to get them to do their dutys . . .” When slaves were incapable of a job, he often hired Dutch or German free hands. When slaves escaped, Durnford sent his overseer to track them down. Of one disobedient slave he wrote, “I ordered five round [lashes] to be given him yesterday . . . He is a wicked fellow.”
Though John McDonogh freed 85 of his blacks and set them up with jobs in Liberia, Durnford thought it was foolish to free slaves, since he thought they could not care for themselves: “There is not one in a hundred that could save money. They have not the moral courage to deprive themselves of luxuries.” During his life he freed only four slaves — a laborer in his 50s and three mulatto children. McDonogh freed all but a few slaves in his will, but Andrew Durnford freed only one at his death — an illegitimate child.
Durnford’s legitimate son was not a kind master to the slaves he inherited. “The race relationship between this mulatto and the slaves may have been more severe than that found between slaves and white owners and overseers,” writes Mr. Whitten. Slavery was, indeed, a vexing question, scarcely illuminated by the clichés with which it is invariably addressed.
| IN THE NEWS |
|---|
O Tempora, O Mores!
Racism in the Ranks
Last December, two white soldiers at Fort Bragg were arrested for killing two blacks in nearby Fayetteville, N.C. One of the soldiers had a Nazi flag and “neo-Nazi” literature in his room, so the incident has provoked a huge, self-righteous hunt for “bigotry” in uniform. The army has issued reports claiming that very few of its boys are members of “extremist” organizations, and says it discharges any who are “active” participants. Now it is considering banning even “passive” participation — simple receipt of literature — even though cooler heads have pointed out that this might violate one of the cherished freedoms the armed forces are supposed to defend.
Meanwhile, race-killings of a different color somehow do not attract attention. On March 5, a Marine Corps sergeant and native of Guam walked into the office of Lt. Col. Daniel Kidd at Camp Pendleton and shot him dead. He also shot Lt. Col. Thomas Heffner and then stopped off to explain his actions to a group of astonished Marines:
I just shot the XO [executive officer] and CO [commanding officer]. I did it for the brotherhood and the brown side. This is only the beginning. We have a hit list. The brothers have been wronged and others are in the pen and more will die unless they are released.
This incident has barely made it into the newspapers, much less prompted an all-out hunt for racists. In the mean time, sources at Fort Bragg suggest that the two “Nazi” soldiers did not kill the two blacks for racial reasons but because of an old-fashioned drug swindle. The blacks reportedly sold them marijuana cut with oregano, but this, too, has somehow failed to become much of a news story. (Samuel Francis, Racism of a More Murderous Hue, Tribune Media Services, March 19, 1996. Tony Perry, Prosecutor Offers Scenario in Marine Officer’s Slaying, Los Angeles Times, March 8, 1996.)
The U.S. 5th Circuit Court of Appeals has ruled that the University of Texas must ignore race when admitting students. The case is a victory for Cheryl Hopwood, a 32-year-old white woman who applied to the University of Texas Law School in 1992. She was rejected, despite scores and grades that were better than all but one of the 41 blacks and all but three of the 55 Hispanics who were admitted.
In 1994, a U.S. district court held only nominally in her favor, granting one dollar in damages. Just before the trial, the law school promised to rejig its racial preferences to keep them constitutional, and the court considered this an acceptable solution.
The new ruling limits preferences strictly to corrections of the university’s own acts of discrimination (does this mean that other rejected whites can reapply and get preferential treatment?) and completely forbids preferences to promote “diversity.” Moreover, the court threatened Texas officials with punitive damages if they continue to give unjustified preferences to non-whites.
Although technically this ruling applies only in the 5th circuit — Texas, Louisiana, and Mississippi — the decision will have a national effect because it is so unambiguous. So far, Supreme Court rulings have discouraged fixed quotas but permitted schools to use race as one of several admissions criteria. The result at University of Texas Law School was typical: All blacks and 90 percent of Hispanics whose records showed achievement at a certain level were admitted; only six percent of white applicants at that level were admitted.
The Supreme Court is likely to rule soon on racial preferences in college admissions. There is a good chance it will support the 5th circuit. (David Savage, U.S. Court Bars Race as Admissions Factor, Los Angeles Times, March 20, 1996, p. A1. David Tell, Diversity Strikes Out, The Weekly Standard, April 2, 1996, p. 9.)
Milk Money
When the California milk industry launched a quirky “Got Milk?” campaign, consumption rose among all groups except Hispanics. The ads do not quite work in Spanish because the phrase “Got Milk?” translates roughly into “Are you lactating?” (Leon E. Wynter, Group Finds Right Recipe For Milk Ads in Spanish, Wall Street Journal, March 6, 1996.)
California State University at Chico recently advertised for “dynamic” applicants for teaching positions. Zaida Giraldo, the school’s affirmative action director complained that the word was associated with white men and not with women or non-whites. The school promptly started advertising for “excellent” teachers. (Courtney Leatherman, Advertisement Spurs Debate Over ‘Dynamic’ Professors, Chronicle of Higher Education, Jan. 5, 1996, p. A17.)
Training the Legal Mind
High school students are taking part in a national mock trial competition, that will culminate in national finals to be held in Pittsburgh in May. The fictional case on which youngsters are to hone their brains involves the murder of a black by white supremacists. The killers have already been convicted on criminal charges, and the students conduct a civil trial in which the head of the “White American Supremacist Party” is accused of inspiring the murder even though he was never even near the crime scene. The case is modeled on the actual trial of Tom Metzger of the White Aryan Resistance, who lost a $12 million civil suit brought on behalf of the family of an Ethiopian man killed by some of Mr. Metzger’s alleged followers. (Frank Zoretich, No Mockery of Justice, it’s Just a Mock Trial, Albuquerque Journal, March 24, 1996, p. A6.)
African Justice
In March, South African villagers near Kruger National Park “necklaced” a baboon. A crowd of about 150 caught the animal, soaked it with gasoline, and set a burning tire around its neck. The baboon was a local resident’s pet but the villagers were convinced it was a witch in disguise. (South Africa ‘Necklace’ Kills Pet Baboon, New York Times, March 18, 1996, p. A2.)
What the Church Hath Joined Together . . .
Two years ago, the United Methodist Church appointed a black preacher, Percy Reeves, to a majority-white congregation in Charlotte, N.C. This was to be a model of full integration for the entire denomination. Instead, the church now rocks to gospel music, people shout “amen” from the pews, and the Nordic-looking portraits of the disciples have come down. During Black History Month, Malcolm X and Jesse Jackson take their places.
Somehow, very few whites attend any more. One of the survivors, Mary Ann Ogle, explains: “When you mesh two cultures — races — it’s a difficult thing to do. More difficult than you can imagine.” (Integration Goes Awry in Charlotte, News and Observer (Raleigh), March 26, 1996.)
Whites Can Be Useful
Over the past fifteen years the white population of Matteson, Illinois has dwindled from 84 to 47 percent. The tax base is shrinking and property values are threatened. To keep the town from getting any blacker, the interracial village council has launched a $65,000 advertising campaign to persuade whites to live in Matteson. One black resident, Rosemary Lomax, who supports the campaign, says, “it’s not about making Matteson lily white. It’s about keeping property values up.” Another black opposes spending the money. “They’ll come back because there really is no place for them to run any more,” he explains. (Don Terry, In White Flight’s Wake, a Town Tries to Keep Its Balance, New York Times, March 11, 1996, p. A12.)
Peddling Juice
O.J. Simpson is angry at major networks for refusing to carry ads for a $30 video which, he claims, proves he is innocent. He says that Marcia Clark, Denise Brown, Christopher Darden, and Faye Resnick have made money selling their versions of the trial, and that the media are preventing him from getting his fair share. Indeed, even Geraldo Rivera and The National Enquirer have rejected the ads as beneath their standards. So far, only Black Entertainment Television is willing to promote Mr. Simpson’s “alibi video.” (Abiola Sinclair, O.J. Simpson complains, ‘They’re getting over on me,’ New York Amsterdam News, Feb. 10, 1996, p.4.)
German Fakery
A 1994 German television documentary showed a group of Germans wearing KKK robes and burning a cross. The producer, Michael Born, now confesses that he got a group of friends to stage the event because he knew the footage would sell. The truth came out when German police mounted a search for the wicked klansmen. (Terrence Petty, German Documentary Producer Faces Charges, Charlotte Observer, Feb. 15, 1996, p. 20A.)
Meanwhile, the Allensbach Institute, Germany’s oldest and best-known opinion polling firm has admitted that it deliberately underpredicted support for the pro-German, anti-immigrant Republican Party. The institute predicted that the party would win only 4.5 percent of the vote in the March 24 elections to the Baden-Württemberg state assembly — just under the minimum five percent required for actual representation. An Allensbach spokesman said the institute did not want to create a band-wagon effect by issuing a more accurate prediction. The party, led at the national level by a former Waffen-SS officer, actually won 9.1 percent of the vote. (Tom Heneghan, Pollsters Slammed for Hushing up German Far-Right, Reuter, April 1, 1996.)
Many third-world immigrants run up huge long-distance phone bills and then stiff the telephone company. They are eventually cut off from service, and the large number of immigrants accounts for why New York City has more households without telephones — 12 percent — than any other American city.
Entrepreneurs have set up storefront telephone businesses where customers pay in advance before they call overseas. Now, a small company called Microtel Communications is installing home telephones that operate on the same principle. For $23 a month, bad credit risks can make local calls, dial 911, and take calls from anywhere. For long distance, however, they must pay cash in advance at a company store. Long-distance service cuts off when the money runs out. The company is doing a brisk business under the slogan, “Todos Califican,” or “everybody qualifies.” (Randy Kennedy, Innovative Telephone Service is Aimed at Immigrants in New York, New York Times, March 18, 1996, p. B12.)
State and federal prisons hold convicts serving sentences of a year or more. Locally operated jails hold people awaiting trail or serving sentences of a year or less. On June 30, 1985, there were 1,104,074 men and women in prison and some 500,000 in jail. This total of approximately 1,600,000 Americans behind bars was a new record. The prison population increased by 89,707 during the preceding 12 months, which was also a record. Between 1980 and 1994, the total number of people in prison and local jails nearly tripled — from 501,886 to 1,483,410.
In 1995, black men were 7.9 times more likely to be in prison that white men, and black women were 7.3 times more likely than white women. Almost seven percent of all black men were in prison compared to less than one percent of white men. In the ten years from 1984 to 1994, the percentage of black men in prison doubled from 3.3 percent to 6.6 percent. The figure for white men also doubled from 0.4 percent to 0.8 percent. However, the Justice Department’s “white” figures include most Hispanics, so black-white disparities are greater than reported.
Race explains much a considerable part of the differences in incarceration rates from state to state. The states with the largest numbers of prisoners per 100,000 population — Texas (659), Louisiana (573), Oklahoma (536), South Carolina (510) — have large minority populations. States with the lowest incarceration rates — North Dakota (90), Minnesota (103), Maine (112), West Virginia (134), Vermont (135) — have few minorities. (Department of Justice Press Release, State and Federal Prisons Report Record Growth During Last 12 Months, Dec. 3, 1995.)
Prejudice and Profit
Though Manhattan’s George Washington High School is running out of books and supplies, it has found the money (after laying off 18 teaching assistants) to combat racism. It has hired the Efficacy Institute to spread the word that low educational achievement by blacks is caused by racist teachers. The seminars cost $10,000 for every 40 people. George Washington High has scheduled 5 seminars for the year, and the New York public school system is considering city-wide implementation. (Lawrence Goodman, Crew: Hire Race Expert, New York Post, Jan. 23, 1996. A costly ‘learning’ experience, New York Post, Feb. 1, 1996.)
Charity Disparity
Many black charities report that the growing numbers of middle-class blacks are increasingly unwilling to make donations. A 1989 study revealed that one third of black households earning between $30,000 and $50,000 donated nothing to charity whereas only one sixth of similar white households donated nothing. Last year, the nation’s top black school, Howard University, received donations from only 4 percent of alumni. By comparison, 28 percent of Vanderbilt University’s alumni contributed — though Vanderbilt made a much greater effort to raise money.
One black fundraiser says it is easier to raise money from whites than from blacks because whites feel guilty. Another black fundraiser accuses black professionals of hypocrisy because they denounce white racism but ignore the needs of poor blacks.
Often, when blacks do give money, it is only to black institutions. One graduate of Hampton University and M.I.T. gives only to Hampton. “My assumption is that whites will take care of white institutions,” he says. A black dentist explains that she gives money to the American Heart Association because “blacks suffer from heart disease at a greater rate than whites.” (Jonathan Kaufman, Black Charities Say Growing Middle Class Isn’t Giving Enough, Wall Street Journal, January 29, 1996, p. A1.)

| LETTERS FROM READERS |
|---|
Sir — I think you have done a great service in the April issue with your treatment of Gunnar Myrdal’s American Dilemma. I have been aware of the book since childhood and have long felt I should read it, but never had the stamina to drag myself through 1,400 pages of Scandinavian English.
There were several things that struck me on reading your excellent article. First, the rot certainly set in long ago, didn’t it? Already in the 1940s, the intellectual climate in the United States was such as to make a spectacular best-seller out of a book that scoffs at racial differences and blames whites for every black failure. If anything, we have a more sober intellectual climate today — one that can make a best-seller out of The Bell Curve.
Second, I think the passages you highlighted that claim we can transform human nature and eliminate human suffering are very, very important. They are an utterly candid statement of the goals and methods of liberalism. Liberals no longer talk openly about transforming human nature, but is that not what they believe they can do?
It requires nothing short of alchemy to make fighter pilots and inventors out of women, responsible married couples out of homosexuals, lawyers and doctors out of feral ghetto children, a constitutional democracy out of Haiti, or a nation out of many races. Despite the abandonment of Myrdal’s extravagant language, the liberal project remains the same: to transform human nature and force every aspect of life into a ruthlessly egalitarian mold. This is nothing short of a declaration of war by the government against the individual.
Of course, the most astonishing transformation has already taken place — that of the American public into a nation of dupes who believe that these fantastic liberal goals may actually be attainable.
Andrew Harding, Tully, New York
![]()
Sir — Gunnar Myrdal is reported to have been a typical socialist, who loved humanity but couldn’t stand human beings. His son, Jan Myrdal, has just written a book about his parents who were both, he claims, cruel egomaniacs.
Sally Ostler, Reading, Pennsylvania
![]()
Sir — I read with great interest your March account of the latest findings in criminology. I was not surprised to learn that even the academics are beginning to abandon the view that criminals can be “rehabilitated.”
Why, though, did Mr. Jackson write nothing about the death penalty? What do the criminologists say about it these days? I bring this up specifically in connection with Mr. Jackson’s apparent sympathy for the view that “three strikes and you’re out” (putting away third-time violent offenders for life) may not be a good idea. He says that by a certain age most men naturally stop committing crimes, and wonders why we have to house “harmless dodderers” at $25,000 a year each.
We don’t have to. After three strikes — three violent offenses against society — you should really be out, that is to say, dead. Anyone actually convicted of three violent felonies has probably committed many more than that. Putting such people to death would be legitimate retribution and a useful deterrent.
Arthur McCracken, Nashville, Tennessee
The book (Crime, edited by James Wilson and Joan Petersilia) says nothing about the death penalty. I should have noted that.
— Thomas Jackson
![]()
Sir — Do many whites really think they are already a racial minority, as you write in “Yet More Numbers” in the April issue? If that is true — and I am not sure it is — it explains some things. One would be the general readiness of people to assume that whites are oppressors. In most ways whites still obviously run the country and if they are actually a minority they are practicing minority rule. People think that’s unfair, and may be willing to think whites maintain power through “racism” if they really are in positions of authority in such disproportionate numbers.
At the same time, crime rates seem less disproportionate to someone who thinks whites are a minority and nonwhites the majority. Blacks and Hispanics may appear to be committing crimes roughly in proportion to their numbers rather than at rates of five to ten times the white rate.
Finally, if whites are already a minority, what’s the use in trying to preserve a European civilization on this continent? The battle is already lost. Also, since the country seems to stumble along more or less tolerably with a non-white majority, what will it matter if the numbers shift a little more against us?
It is easy to understand where this illusion of minority status comes from. The media are constantly whooping up non-whites and are preoccupied with their problems. But the resulting impression of already being outnumbered is a dangerous source of demoralization for our people.
John Pettim, Madison, Wisconsin